Emergency Ortho: Shoulder
The Shoulder
ATRAUMATIC SHOULDER PAIN:

By far and away this is going to be shoulder impingement syndrome which is really a catch all for subacromal bursitis and/or supraspinatus tendonitis. This is further discussed below. One hallmark for this is pain at night sleeping on the affected side and exam shows pain with anything that decreases the space in the subacromial area (i.e. empty can and Hawkins maneuver). Other subtle diagnoses to consider would also include proximal biceps tendonitis with pain in the same area but instead a Speed's test is positive or just resisted elbow flexion and supination (remember the biceps is the primary supinator) causes pain. If there is bruising and a Popeye arm deformity consider a biceps muscle or tendon rupture. Biceps tendon rupture can be proximal or distal so a patient may present with anterior shoulder pain and have the muscle deformity there. Patients can also have tendonitis of any of the other rotator cuff muscles (remember your SITS muscles), but this is much less common. Mostly document good movement of these muscles to assess for adhesive capsulitis. This can be done with the lift off test and resisted external rotation with arms at sides and elbows at 90 degrees. A full list of special tests can be found on Medscape.

What to document:
R or L hand dominant (arthritis/bursitis) more likely on overused side
Pain at night and with overhead movement, think impingement
Any biceps deformity or pain on exam could indicate a biceps etiology
Speed's test is for proximal biceps tendonitis and should be done while palpating the proximal tendon in the bicipital groove. It can also indicate a labral tear as this is where the long head of the biceps tendon inserts.
Empty can test decreases subacromial space and is for impingement syndrome. A painful Neer's impingment or Hawkin's test do the same.
Test internal and external rotation of the shoulder as well with the lift off test (dorsum of hand on low back and lifted off) and the resisted internal rotation with the arm abducted and elbow at 90 degrees.
Feel a radial pulse and test elbow and wrist flexion/extension
A frozen shoulder (adhesive capsulitis) will have decreased ROM passively, many other etiologies can have decreased active ROM due to pain.
What to do:
A sling is fine in the short term but can lead to frozen shoulder particularly in the elderly.
Encourage early ROM exercises like pendulum swing.
Often pain will be chronic and need a PT referral, inform patient to f/u with PCP or orthopedist if not improved with conservative measures.
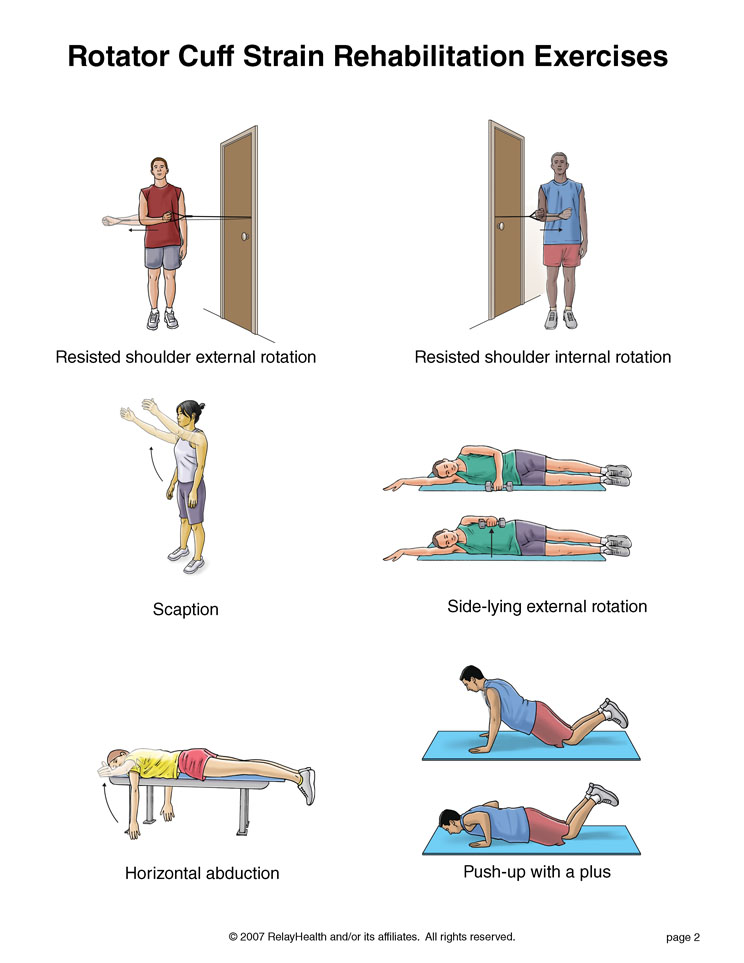
Strengthening of the rotator cuff muscles is helpful in many conditions so as long as not worsening pain with the exercises start rotator cuff muscle strengthening. This is a reasonably good educational video for patients and providers to treat impingement syndrome.
This is another great guide for shoulder rehab that you can print and send home with patients.
What not to miss:
A complete rotator cuff tendon tear. This will usually be the supraspinatus muscle and patient will not be able to abduct the first 15 degrees. They may compensate with shoulder hiking and will have a positive arm drop.
Biceps pathology such as a tear that may delay appropriate diagnosis and treatment.
Any neurologic or vascular injury.
Of course, any medical diagnosis (such as ACS) that might mimic or have associated shoulder pain. A good history and PE should clear this up so be thorough.
TRAUMATIC SHOULDER INJURY:
Be sure to get a Y view as pointed out by this great article on posterior dislocation on LifeInTheFastLane.com
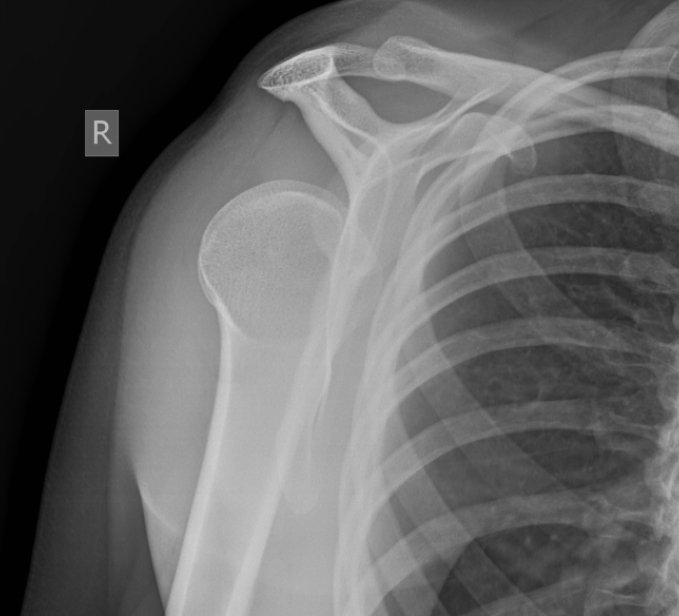
Hard to miss a glenohumoral dislocation or humoral neck fracture (BTW it's the surgical neck not the true humoral neck) on x-ray. Except for a posterior dislocation which can be missed on just an AP view (see image right). Also because there are a bunch of different ways to reduce a shoulder, I won't go into the debate here, but just know if there are multiple ways to do something there is no one best way so find a technique and get good at it. Subtleties to these exams include documenting sensation over the lateral deltoid which shows the axillary nerve is functioning as it is often damaged with dislocation or fracture. Of course, always document neuro and vascular status distally as the brachial artery and the arm nerves run close to the humerus. A clavicle fracture is the most common of all the traumatic shoulder injuries and should be evident on exam and confirmed on x-ray. I've never met one that couldn't go home for outpatient follow-up but check to make sure it's not an open fracture or the skin is tented and blanching and soon to be an open fracture. Those would need immediate surgical reduction. An AC joint separation, can be difficult to pick up on plain films so consider looking at the contralateral side for comparison and if mechanism and exam is strongly indicative my be a grade I. Knowing the grades of AC joint separation not all that important as you could sling them all and send them to ortho outpatient.
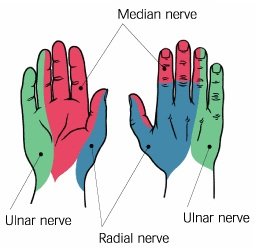
Having a quick neuro exam of the hand/fingers is a good way to ensure proximal peripheral nerve function is okay. You can make up your own or memorize this quick exam of the nerves of the arm
Radial nerve: sensation = dorsal hand, webspace between thumb and index finger; action = elbow/wrist/finger extension
Median nerve: sensation = radial border of the index finger; action = thumb abduction (thumb to index finger)
Ulnar nerve: sensation = ulnar border of the 5th finger; action = fifth finger abduction (spread the fingers)
Musculocutaneous nerve: sensation = mid lateral forearm; action = elbow flexion with supination (to isolate the biceps brachii)
Axillary nerve: sensation = over insertion of the deltoid muscle; action = shoulder abduction
Bonus: pinch the thumb on the fifth finger to assess median and ulnar nerve motor function at the same time!!!
What to document:
Complete neuro exam: discussed above
Vascular exam including distal pulses and capillary refill.
Bony tenderness or deformity (compare to contralateral side). This should include at a minimum cervical spine, spine of the scapula, clavicle, AC joint, acromium
Soft tissue deformity, or lack thereof. Classically the squaring of the deltoid with anterior dislocation.
Active and passive ROM. If any intervention such as reduction is performed document ROM before and after.
What to do:
Get X-rays duh! Probably not a good idea to try to reduce a supposed dislocation that is really a fracture.
Treat for pain. Sometimes moving the joint for radiographs and of course interventions such as reduction need appropriate pain control up to procedural sedation.
Call for expert advice in anything that you don't routinely handle. My rule of thumb is call a consultant surgeon for anyone that is going to eventually need surgery.
What not to miss:
Nerve or vascular injury. Particularly fractures can lacerate important structures like an artery. The axillary nerve (see below) is the most common nerve injury from dislocation. It provides sensation of the lateral deltoid. Document sensation here before the patient goes home (that means before and after reduction).
Secondary injury such as head or neck. If there is enough force to dislocate or fracture then perform a full physical (such as an ATLS secondary survey) to look for concomitant injuries.
Example documentation of the PE:
Musculoskeletal: The *** shoulder is *** swollen or deformed on inspection. The range of motion is full/limited to *** because of the pain. There is good abduction without shoulder hiking and no arm drop when compared to the contralateral side. There is *** tenderness of the clavicle, a.c. joint, or spinous scapula. There is *** tenderness inferior to the acromion in the area of the supraspinatus tendon and bursa. Empty can test is ***. Hawkin's test and Neer impingement test is ***. Speed's test is ***. There is *** internal and external rotation as tested by lift off and resisted external rotation with arm in adduction. Sensation intact over the lateral deltoid and down to the fingertips including the palm and dorsum of the hand. Positive radial pulse. Normal range of motion and 5+ strength to flexion and extension of the wrist and elbow. Fingers are warm and well perfused with good capillary refill.