
CC: CP - the ECG (STEMI)

ECG
The ElectroCardioGram
Obviously, almost everything in EM cardiology starts with an EKG, and we also know that anyone with a chest and pain somewhere in the body will get an EKG from the triage nurse. Just think of that last patient you saw with finger pain who said, "I read online that this could mean a heart attack.”
In my experience, the difficulty in cardiac patients in the ED is not in those that present with a grossly abnormal EKG showing a STEMI. These patients can be diagnosed by EMS and essentially, present with a disposition. Give aspirin and your hospital's preferred antiplatelet, call cardiology, and ship them to the cath lab. No, the challenge in emergency medicine is patients without obvious ischemic findings on their EKG, figuring out who to work up and pursue further testing, and keeping in your differential all the other important cardiac pathologies that could masquerade as other diseases.
Not that you are allowed to miss a STEMI, so here is a quick review below, along with other STEMI equivalents or subtle changes that can indicate myocardial injury.
The ST-segment Elevated Myocardial Infarction (STEMI)

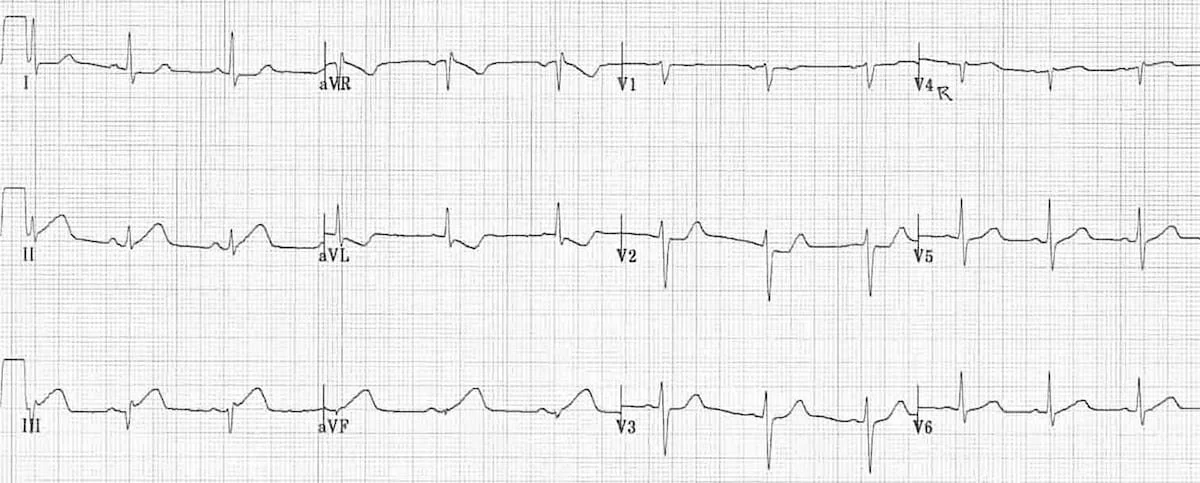
Figure 8. Electrocardiogram example of ST-segment elevation. The initial onset of the Q wave shown by arrow 1 serves as the reference point and arrow 2 shows the onset of the ST-segment or J-point. The difference between the two identifies the magnitude of displacement. Measurements of both arrows should be made from the top of the electrocardiogram line tracing.
STEMI is described in the Fourth Universal Definition of Myocardial Infarction as the following (in the absence of LVH or BBB)
New ST Elevation at the J point of at least 1 mm in two contiguous leads (except for V2-V3, see below)
In leads V2-V3, ST elevation at the J point must be
≥2 mm in men over 40 or ≥2.5mm in men under 40 y/o
≥1.5mm in women regardless of age
Wait, what are contiguous leads??? Contiguous leads are:
For the precordial leads, it is the neighboring leads (V1-V2 Septal, V3-V4 Anterior, V5-V6 Lateral)
II, III, and AVF are contiguous leads for the inferior portion of the myocardium
I and AVL are contiguous leads for the high lateral portion of the heart (this one is often forgotten)
For the posterior leads, V7, V8 and V9 are contiguous leads

“In those patients with conduction disturbances including bundle branch blocks the Fourth Definition of MI states, “Ischemic symptoms, and presumed new LBBB or right bundle branch block (RBBB) that is not rate-related, are associated with an adverse prognosis. In patients with LBBB, ST-segment elevation ≥1 mm concordant with the QRS complex in any lead may be an indicator of acute myocardial ischemia. Similar findings can be useful in detecting ECG evidence for acute myocardial ischemia in patients with right ventricular paced rhythm.”
I find it best to simply look up the Sgarbossa criteria or the Smith-Modified Sgarbossa Criteria in any patient with a LBBB or pacer:
Concordant ST elevation ≥ 1 mm in ≥ 1 lead
Concordant ST depression ≥ 1 mm in ≥ 1 lead of V1-V3
Proportionally excessive discordant STE in ≥ 1 lead anywhere with ≥ 1 mm STE, as defined by ≥ 25% of the depth of the preceding S-wave"
That does not account for a new RBBB, so if this is ever the case, an old ECG showing RBBB is essential to document or consider consulting cardiology if there is a new RBBB.
For more review, here are some “classic” STEMI patterns from Life in the Fastlane:




Other “classic” patterns that you should know include:
“Tombstone T-waves”
ST-depression
New T wave inversions
Other important ECG changes to know:
Anterior-inferior STEMI due to occlusion of a “wraparound” LAD. This presents with simultaneous ST elevation in the precordial and inferior leads, due to occlusion of a variant (“type III”) LAD that wraps around the cardiac apex to supply both the anterior and inferior walls of the left ventricle
Left main coronary artery stenosis: widespread ST depression with ST elevation in aVR ≥ V1
Wellens syndrome: deep precordial T wave inversions or biphasic T waves in V2-3, indicating critical proximal LAD stenosis (a warning sign of imminent anterior infarction)
De Winter T waves: upsloping ST depression with symmetrically peaked T waves in the precordial leads; a “STEMI equivalent” indicating acute LAD occlusion.
What I document (to remind myself of possible ischemic patterns):
*** rhythm, *** rate. PR interval *** ms, QRS *** ms, and QTc *** ms. *** ST-segment elevation or hyper-acute T waves. *** new ST depression. There were *** T wave inversions compared to prior EKG.
Posterior MI considered with no ST depression in V1-V3. ECG examined for Wellen syndrome - no deep precordial T wave inversions or biphasic T waves in V2-3 and De Winter T waves - no upsloping ST depression with peaked T waves in precordial leads. Sgarbossa criteria considered if LBBB/paced ECG. A large S wave in lead I, a Q wave in lead III, and an inverted T wave in lead III seen in acute right heart strain *** seen. Electrical alternans suspicious for large pericardial effusion *** present.
Independently viewed by attending MD and read by me at the bedside.
The second paragraph acts as a reminder of important patterns that could suggest ischemia. Many times I delete this entirely, but it is much faster for me to quickly review this text and delete it, than to go look up.